Loading page, please wait…
Lymphatic Filariasis - UPSC Social Issues
What is Lymphatic Filariasis in UPSC Social Issues?
Lymphatic Filariasis is a key topic under Social Issues for UPSC Civil Services Examination. Key points include: Lymphatic Filariasis (LF), or elephantiasis, is a neglected tropical disease caused by filarial parasites transmitted by mosquitoes.. India faces a significant LF burden, with 345 endemic districts across 20 states/UTs, necessitating large-scale interventions.. The Bi-annual Nationwide Mass Drug Administration (MDA) campaign is a key strategy to eliminate LF by interrupting transmission.. Understanding this topic is essential for both UPSC Prelims and Mains preparation.
Why is Lymphatic Filariasis important for UPSC exam?
Lymphatic Filariasis is a Medium-level topic in UPSC Social Issues. It is tested in both Prelims (factual MCQs) and Mains (analytical answer writing). Previous year UPSC questions have frequently covered aspects of Lymphatic Filariasis, making it essential for comprehensive IAS preparation.
How to prepare Lymphatic Filariasis for UPSC?
To prepare Lymphatic Filariasis for UPSC: (1) Study the comprehensive notes covering all key concepts on Vaidra. (2) Practice previous year questions on this topic. (3) Connect it with current affairs using daily updates. (4) Revise using key takeaways and mind maps available for Social Issues. (5) Write practice answers linking Lymphatic Filariasis to related GS Paper topics.
Key takeaways of Lymphatic Filariasis for UPSC
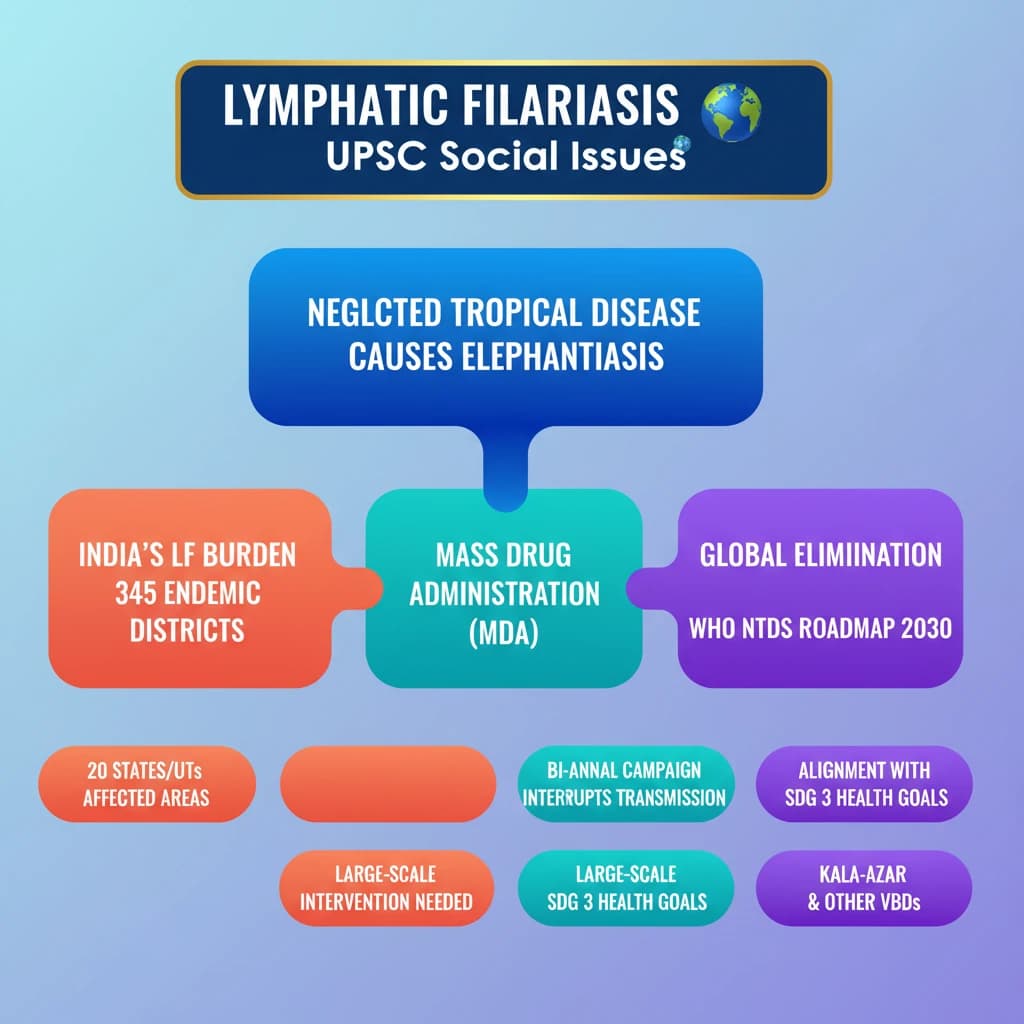
- Lymphatic Filariasis (LF), or elephantiasis, is a neglected tropical disease caused by filarial parasites transmitted by mosquitoes.
- India faces a significant LF burden, with 345 endemic districts across 20 states/UTs, necessitating large-scale interventions.
- The Bi-annual Nationwide Mass Drug Administration (MDA) campaign is a key strategy to eliminate LF by interrupting transmission.
- The National Vector Borne Disease Control Programme (NVBDCP) is an umbrella program managing LF, Kala-Azar, and other vector-borne diseases.
- India's efforts to eliminate LF and Kala-Azar align with WHO's NTDs Roadmap 2030 and contribute to SDG 3.
- Integrated approaches, including vector control, housing improvement (PMAY-G), and ASHA network mobilization, are crucial for effective disease control.
Lymphatic Filariasis
Medium⏱️ 12 min read
social issues
📖 Introduction
Introduction to Lymphatic Filariasis
Recently, the Union Minister of State for Health and Family Welfare launched the first phase of the Bi-annual Nationwide Mass Drug Administration (MDA) campaign for Lymphatic Filariasis (LF) elimination. This initiative underscores India's commitment to eradicating neglected tropical diseases.
What is Lymphatic Filariasis?
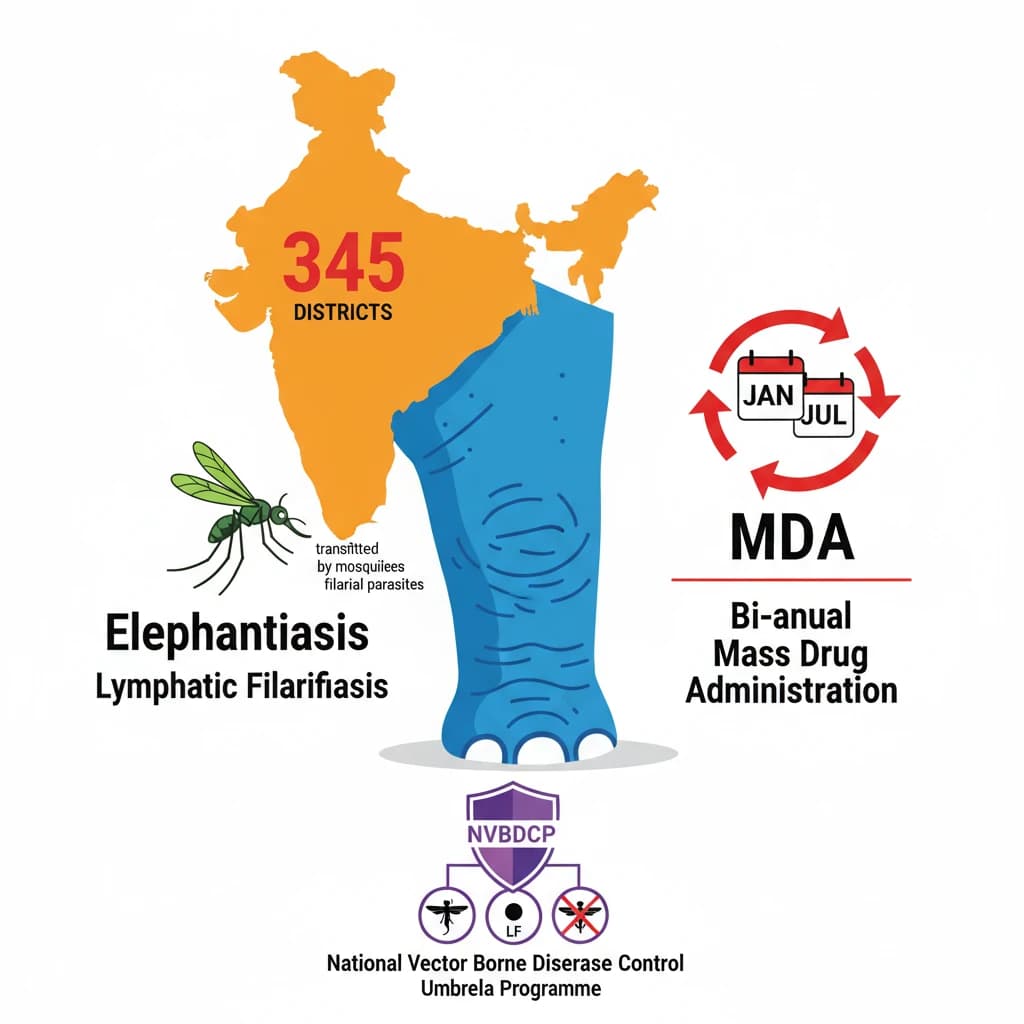
Lymphatic Filariasis (LF), commonly known as elephantiasis, is a debilitating neglected tropical disease (NTD). It is caused by infection with filarial parasites which are transmitted to humans through mosquito bites.
Definition: Lymphatic Filariasis is a parasitic disease caused by thread-like worms that block the lymphatic system, leading to severe swelling and disfigurement, primarily in the limbs and genitals.
Global and National Prevalence of LF
In 2021, approximately 882.5 million people across 44 countries lived in areas requiring preventive chemotherapy. This highlights the widespread global burden of Lymphatic Filariasis.
In India, LF remains a serious public health challenge. Currently, there are 345 Lymphatic Filariasis endemic districts spread across 20 states and union territories.
- Approximately 75% of the Mass Drug Administration (MDA) districts are concentrated in five states: Bihar, Jharkhand, Uttar Pradesh, Odisha, and Telangana.
- The disease is more prevalent among the urban poor but also significantly affects all segments of the rural population.
India's Recent Initiative: Mass Drug Administration (MDA) Campaign
The recently launched Bi-annual Nationwide MDA campaign aims to interrupt disease transmission. It achieves this by providing free preventive medications to residents in affected areas.
MDA Campaign Goal: To check disease transmission by administering preventive medications. The initial phase of the campaign is set to cover 92 districts across 11 states.
Related Neglected Tropical Disease: Kala-Azar
While the primary topic is Lymphatic Filariasis, the source material also details aspects of Kala-Azar, another significant neglected tropical disease in India. Control efforts for various vector-borne diseases often share common strategies and programmatic frameworks.
Diagnosis and Treatment of Kala-Azar
Suspected cases of visceral leishmaniasis, commonly known as Kala-Azar, require immediate medical attention. Diagnosis involves assessing clinical signs combined with specific parasitological or serological tests.
Mortality Rate: If left untreated, Kala-Azar can be fatal in 95% of cases, underscoring the urgency of early intervention.
Prevention and Control of Kala-Azar
Effective prevention and control strategies are crucial for reducing the prevalence of Kala-Azar, preventing disabilities, and saving lives.
- Early Diagnosis and Prompt Treatment: These are paramount in reducing disease burden and preventing severe outcomes.
- Vector Control: Measures such as insecticide spray and the use of insecticide-treated nets help reduce transmission by decreasing the population of sandflies, the disease vector.
- Effective Disease Surveillance: This is vital for monitoring disease trends, detecting epidemics early, and responding effectively to high case fatality rates.
- Social Mobilization and Partnerships: Community education and strong collaboration with various stakeholders are essential for successful control programs.
India’s Efforts to Control Kala-Azar
The Government of India has a long-standing commitment to eliminating Kala-Azar through various programmatic interventions.
- The government launched a centrally sponsored Kala-azar control program in 1990-91, which was subsequently revised in 2015.
- The program aimed to eliminate Kala-azar by 2023, aligning with the WHO neglected tropical diseases (NTDs) Roadmap goal of 2030.
National Vector Borne Disease Control Programme (NVBDCP), 2003: This is an umbrella program that oversees the prevention and control of multiple vector-borne diseases, including malaria, lymphatic filariasis, kala-azar, and chikungunya.
Recent Efforts Against Kala-Azar
Recent initiatives have focused on multi-pronged strategies to combat Kala-Azar effectively.
- Indoor Residual Spraying: Rigorous efforts are made to curtail sandfly breeding sites through indoor residual spraying. A special soil is also applied to seal crevices in mud walls, preventing sandflies from nesting.
- Housing Improvement: Pucca houses have been constructed in Kala-Azar affected villages under the Pradhan Mantri Awaas Yojana-Gramin (PMAY-G). A total of 25,955 houses were built in 2017-18 (11,371 in Bihar & 24,584 in Jharkhand).
- ASHA Network Mobilization: The Accredited Social Health Activist (ASHA) network is mobilized to ensure the completion of treatment for Post-Kala-Azar Dermal Leishmaniasis (PKDL) patients, who require a 12-week course of Miltefosine (an antileishmanial agent).
Post-Kala-Azar Dermal Leishmaniasis (PKDL)
PKDL is a skin condition that can follow an episode of visceral leishmaniasis (Kala-Azar). It manifests as rashes on the face, arms, and trunk.
Prevalence: PKDL primarily affects regions like Sudan and the Indian subcontinent, with 5-10% of Kala-Azar patients developing this condition.
PKDL may appear 6 months to a year after the completion of Kala-Azar treatment. Importantly, individuals with PKDL can potentially serve as a reservoir, spreading Leishmania parasites.
💡 Key Takeaways
- •Lymphatic Filariasis (LF), or elephantiasis, is a neglected tropical disease caused by filarial parasites transmitted by mosquitoes.
- •India faces a significant LF burden, with 345 endemic districts across 20 states/UTs, necessitating large-scale interventions.
- •The Bi-annual Nationwide Mass Drug Administration (MDA) campaign is a key strategy to eliminate LF by interrupting transmission.
- •The National Vector Borne Disease Control Programme (NVBDCP) is an umbrella program managing LF, Kala-Azar, and other vector-borne diseases.
- •India's efforts to eliminate LF and Kala-Azar align with WHO's NTDs Roadmap 2030 and contribute to SDG 3.
- •Integrated approaches, including vector control, housing improvement (PMAY-G), and ASHA network mobilization, are crucial for effective disease control.
🧠 Memory Techniques
95% Verified Content
📚 Reference Sources
•World Health Organization (WHO) reports on Neglected Tropical Diseases (NTDs)
•Ministry of Health & Family Welfare, Government of India official releases